
Degenerative Mitral Valve Disease in Dogs
Degenerative mitral valve disease, also called myxomatous mitral valve disease (MMVD/DMVD), is the most common acquired heart disease in dogs. It most often affects small- to medium-breed dogs, including Cavalier King Charles Spaniels, Dachshunds, Chihuahuas, Poodles, Maltese, Shih Tzus, and mixed small-breed dogs. Among these, Cavalier King Charles Spaniels are uniquely predisposed, often developing disease at a younger age with more rapid progression, consistent with a strong genetic component.
In DMVD, the mitral valve becomes thickened, irregular, and leaky. Over time, this leak can cause enlargement of the left atrium and left ventricle. Some dogs remain stable for years, while others progress to congestive heart failure (CHF).
The goal of diagnosis and treatment is to identify the stage of disease, determine whether medication is needed, monitor for progression, and discuss advanced options when appropriate.

What Is the Mitral Valve?
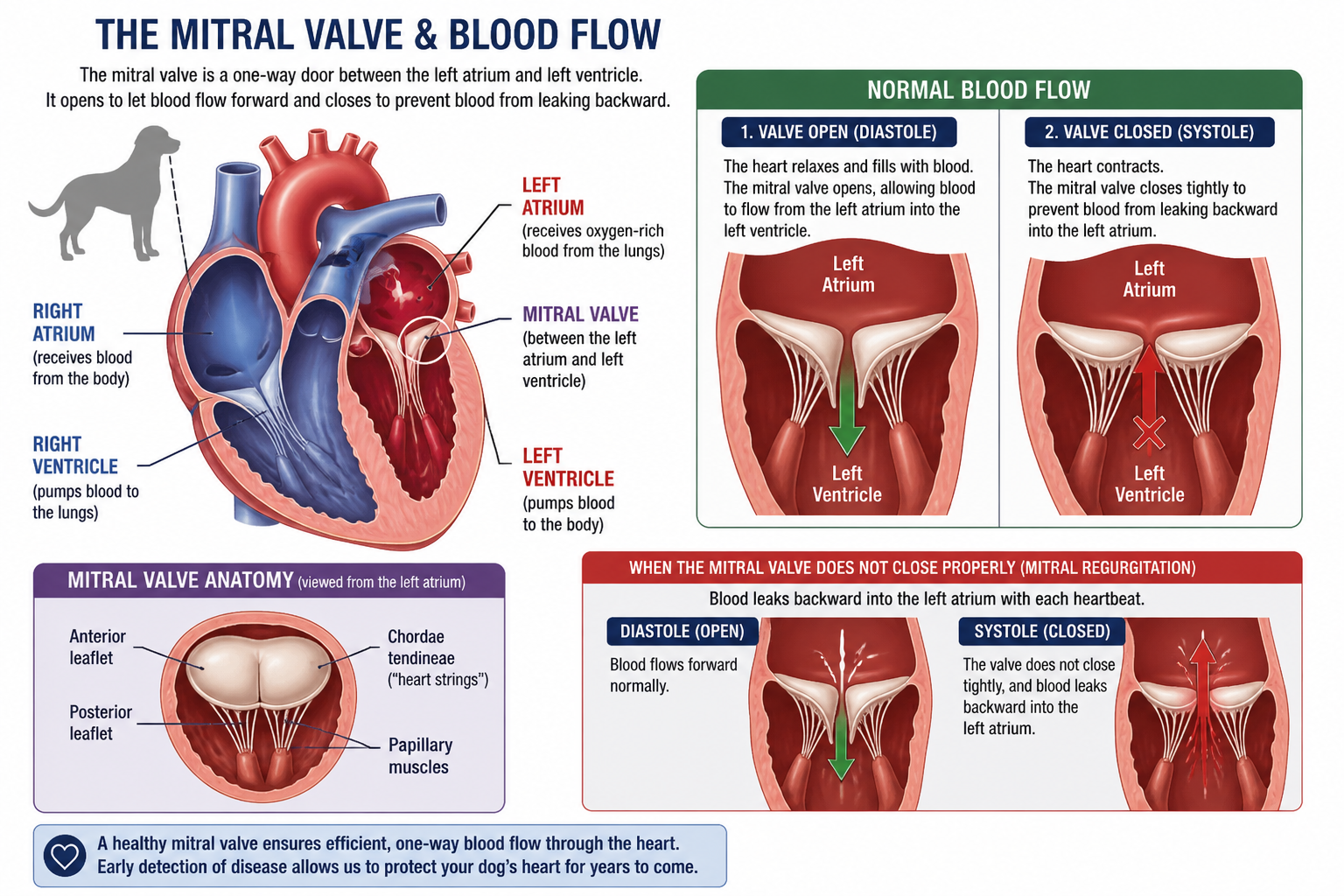
The mitral valve is an atrioventricular valve located between the left atrium and left ventricle. It is made up of two leaflets, along with supporting structures including the chordae tendineae and papillary muscles, which help keep the valve stable during the cardiac cycle.
Its primary role is to maintain one-way blood flow. During diastole (when the heart relaxes), the valve opens to allow blood to flow from the left atrium into the left ventricle. During systole (when the heart contracts), it closes tightly to prevent blood from leaking backward into the atrium as blood is pumped out to the body.
Epidemiology and Pathophysiology
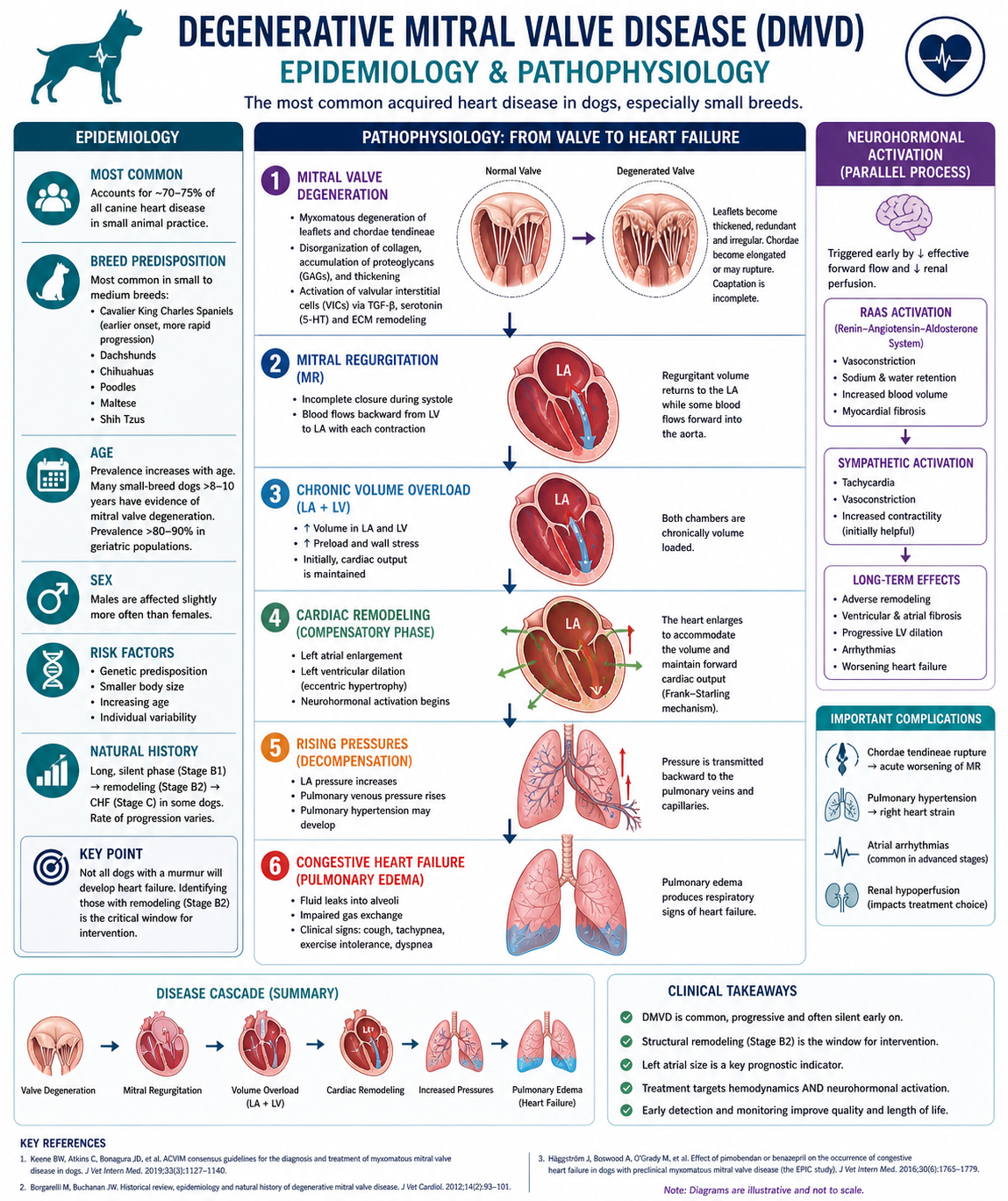
The prevalence of DMVD increases significantly with age. While uncommon in young dogs (outside of predisposed breeds), a large proportion of small-breed dogs over 8–10 years of age will have evidence of mitral valve degeneration, with prevalence estimates exceeding 80–90% in geriatric populations. Despite this, the clinical course is highly variable—many dogs remain asymptomatic for years, while others progress to congestive heart failure. Males are slightly overrepresented, and smaller body size is consistently associated with increased risk.
Degenerative mitral valve disease is characterized by progressive myxomatous degeneration of the mitral valve apparatus, involving the valve leaflets, chordae tendineae, and supporting structures. Histologically, this process is marked by disorganization of collagen fibers, expansion of the spongiosa layer, and accumulation of proteoglycans and glycosaminoglycans, leading to thickened, redundant, and weakened valve leaflets.
At a cellular level, there is activation of valvular interstitial cells (VICs), which undergo a phenotypic shift toward a myofibroblast-like state. This transformation is driven by signaling pathways including TGF-β (transforming growth factor-beta), serotonin (5-HT), and extracellular matrix remodeling pathways, contributing to progressive structural degeneration of the valve.
Functionally, these changes result in incomplete coaptation of the mitral valve leaflets during systole, often accompanied by elongation or rupture of the chordae tendineae. The consequence is mitral regurgitation (MR), where a portion of left ventricular stroke volume is ejected backward into the left atrium.
This regurgitant flow creates a state of chronic volume overload affecting both the left atrium and left ventricle. In response, the heart undergoes eccentric hypertrophy, characterized by chamber dilation with relatively preserved wall thickness. The left atrium enlarges to accommodate increased volume and maintain lower filling pressures, while the left ventricle dilates to preserve forward cardiac output via the Frank-Starling mechanism.
Over time, however, these compensatory mechanisms become maladaptive. Progressive left atrial enlargement leads to increased left atrial pressure, which is transmitted backward into the pulmonary veins and capillary beds. Once pulmonary capillary hydrostatic pressure exceeds oncotic pressure, pulmonary edema develops, marking the onset of congestive heart failure.
In parallel, chronic mitral regurgitation results in neurohormonal activation, including the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system. While initially compensatory—supporting blood pressure and perfusion—these pathways promote vasoconstriction, sodium and water retention, myocardial remodeling, and fibrosis, further exacerbating disease progression.
Additional pathophysiologic contributors may include:
Chordae tendineae rupture, leading to acute worsening of mitral regurgitation
Pulmonary hypertension, secondary to chronic elevation in left-sided filling pressures
Atrial arrhythmias, due to structural and electrical remodeling of the left atrium
How Degenerative Mitral Valve Disease (DMVD) Is Diagnosed
Diagnosing degenerative mitral valve disease involves combining findings from the physical exam, imaging, and clinical signs. No single test provides the full picture—the goal is to determine both whether disease is present and how advanced it is.
Physical Examination
A heart murmur is often the first indication of DMVD. A heart murmur is an abnormal sound heard during a heartbeat, caused by turbulent blood flow within the heart or great vessels. Instead of the normal “lub-dub” sounds, a murmur creates a whooshing or swishing noise when listened to with a stethoscope. It is typically heard best on the left side of the chest (left apical systolic murmur) and represents turbulent blood flow across the mitral valve.
Murmur intensity may increase as disease progresses, but it does not reliably reflect disease severity or stage on its own. Further diagnostics are always needed to determine whether treatment is indicated.
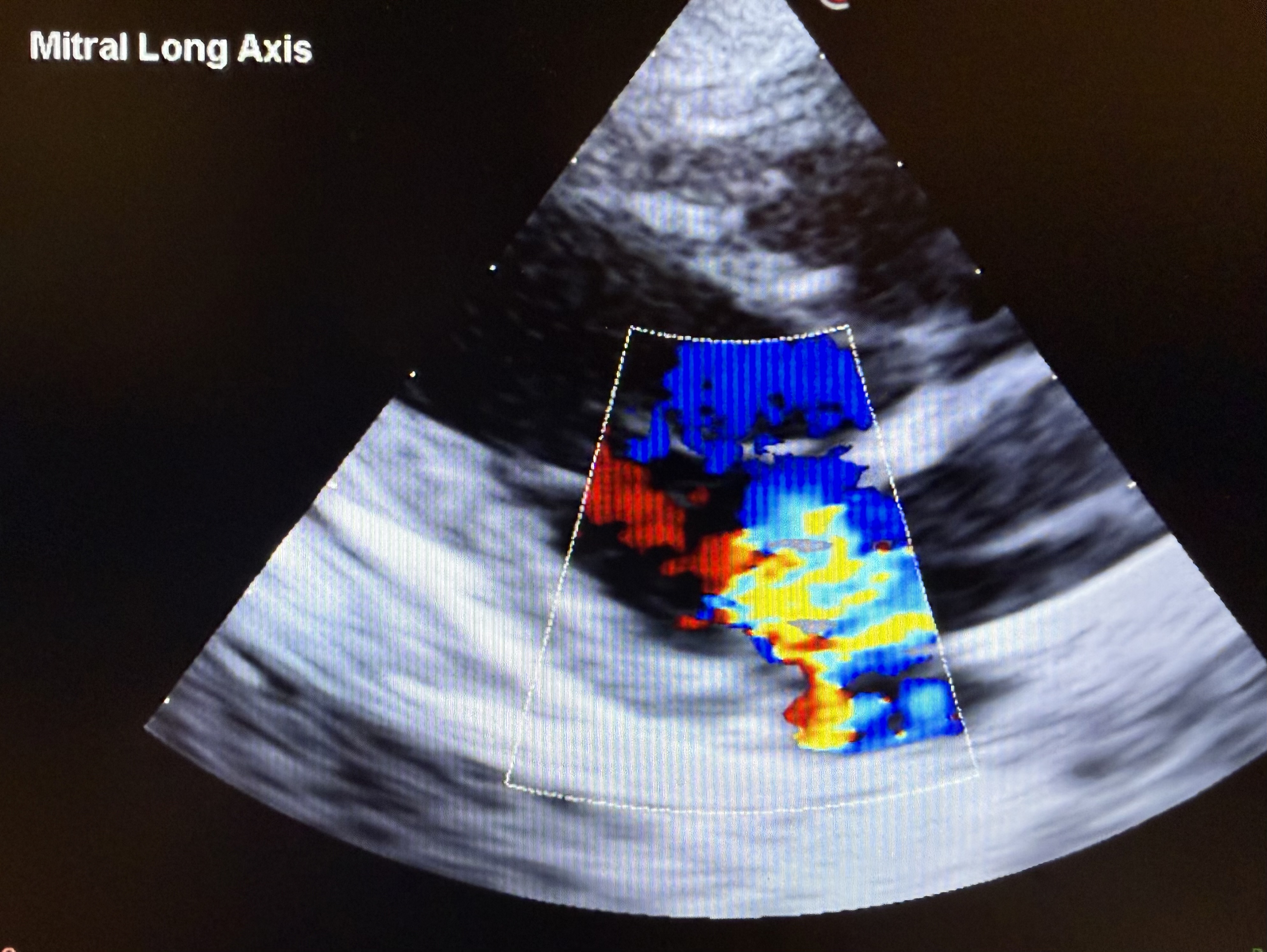
🫀 Echocardiography
Echocardiography is the gold standard test for diagnosing and staging degenerative mitral valve disease.
It is a non-invasive imaging test that uses ultrasound to create real-time images of the heart, allowing direct assessment of both structure and function.
An echocardiogram provides detailed information about:
Mitral valve structure
Thickening, prolapse, or flail leaflets consistent with degenerative diseaseMitral regurgitation
Color Doppler is used to identify and assess backward blood flow across the valveCardiac chamber size
Left atrial size (LA:Ao ratio)
Left ventricular size and function (LVIDdN, FS, EF)
These values help determine whether a dog is in Stage B1 or B2, which directly impacts whether medications like pimobendan +/- ACEIs are recommended.
Cardiac function
Evaluation of systolic performance and overall hemodynamicsOther
Pulmonary hypertension
Chordae tendineae rupture
Changes in other valves or chambers
Thoracic Radiographs (Chest X-Rays)
Thoracic radiographs are a key diagnostic tool in dogs with suspected degenerative mitral valve disease, particularly for determining whether congestive heart failure (CHF) is present.
Key radiographic assessments include:
Vertebral Heart Score (VHS): estimates overall heart size
Vertebral Left Atrial Size (VLAS): improves detection of left atrial enlargement, especially in earlier disease
Cardiac silhouette changes: consistent with left atrial and ventricular remodeling
Pulmonary veins: enlargement suggests increased left-sided filling pressures
Lung patterns: interstitial to alveolar changes consistent with pulmonary edema
Clinical interpretation highlights:
Pulmonary edema on radiographs confirms Stage C (CHF)
Cardiomegaly alone does not indicate heart failure
Radiographs are essential for differentiating cardiac vs respiratory causes of coughing
Findings should always be interpreted alongside clinical signs and echocardiographic data
Limitations:
Do not evaluate mitral valve structure or regurgitation severity
Less sensitive than echocardiography for early cardiac enlargement
Thoracic radiographs—especially when incorporating VHS and VLAS—are essential for assessing heart size and confirming CHF, making them a critical part of staging and management in DMVD.
Degenerative Mitral Valve Disease Staging
Staging is the foundation of managing DMVD. It moves the focus away from the presence of a murmur and toward what actually matters: structural change, clinical status, and risk of progression.
The staging system from the American College of Veterinary Internal Medicine divides disease into four main categories, each with different implications for monitoring and treatment.
Stage A — At Risk
Dogs are predisposed to DMVD but have no evidence of disease.
No murmur
No structural changes
Common in predisposed breeds
👉 Management: No treatment; routine monitoring
Stage B — Structural Disease Without Heart Failure
DMVD is present, but there are no clinical signs of congestive heart failure.
Stage B1 — No Cardiac Enlargement
Murmur present
Heart size within normal limits
👉 Management: Monitor over time (No routine medication)
Stage B2 — Cardiac Enlargement Present
Left atrial and/or ventricular enlargement
Typically defined by:
LA:Ao ≥ 1.6
LVIDdN ≥ 1.7
Increased VHS / VLAS
No clinical signs
👉 Management: Initiate pimobendan
📚 EPIC Trial Insight:
The EPIC study demonstrated that in dogs with Stage B2 DMVD, pimobendan prolonged the time to onset of congestive heart failure or cardiac-related death by approximately 15 months compared to placebo.
This represents a significant clinical impact, effectively extending the asymptomatic period and delaying disease progression.
👉 This makes Stage B2 the most important window for intervention
Boswood A, Häggström J, Gordon SG, et al.
Effect of Pimobendan in Dogs with Preclinical Myxomatous Mitral Valve Disease and Cardiomegaly (EPIC Study).
Journal of Veterinary Internal Medicine. 2016;30(6):1765–1779.
🔗 https://pubmed.ncbi.nlm.nih.gov/27678080/
Stage C — Congestive Heart Failure
Dogs have current or prior evidence of CHF.
Pulmonary edema on radiographs
Clinical signs (tachypnea, dyspnea, sometimes cough)
👉 Management:
Medical therapy, typically including:
Pimobendan
Diuretics (furosemide)
RAAS modulation - ACEI, Spironolactone
Stage D — Refractory Heart Failure
CHF is difficult to control despite standard therapy.
Persistent or recurrent pulmonary edema
Increasing medication requirements
Switching tp torsemide
👉 Management:
Advanced medical strategies
Consideration of referral or interventional options
Quality-of-life discussions
Why Staging Matters
A murmur alone does not determine treatment
Structural changes (B2) identify the window for early intervention
CHF (Stage C) requires objective confirmation with radiographs
Treatment decisions are stage-dependent—not symptom-based alone
Common Cinical Signs of Degenerative Mitral Valve Disease (DMVD) in Dogs
Many dogs with early degenerative mitral valve disease have no obvious symptoms. The condition is often first identified during a routine exam when a veterinarian detects a heart murmur.
As the disease progresses, clinical signs may develop due to increasing cardiac workload, reduced forward blood flow, and/or fluid accumulation in the lungs (congestive heart failure).
Possible Signs as Disease Progresses
Increased resting or sleeping respiratory rate (RR)
One of the earliest and most sensitive indicators of developing congestive heart failureIncreased respiratory effort (RE)
Subtle abdominal push, flared nostrils, or labored breathingExercise intolerance
Tires more quickly, less willing to play or go on walksRestlessness, especially at night
May reflect discomfort or difficulty breathing when lying downDifficulty breathing (dyspnea)
A more advanced and urgent signFainting or collapse (syncope)
Less common; may be related to arrhythmias or advanced diseaseAbdominal distension
Occurs in advanced disease or with right-sided involvement
Monitoring at Home: Sleeping RR & RE
One of the most valuable tools for early detection is monitoring your dog’s sleeping respiratory rate (RR) and respiratory effort (RE).
How to Measure
Count breaths when your dog is asleep or deeply resting
One breath = in + out
Count for 15–30 seconds and multiply to get breaths per minute
What’s Normal?
Typically < 30 breaths per minute when sleeping
Each dog has its own baseline—trends matter more than a single number
When to Be Concerned
Consistent increase above baseline
RR persistently > 30–35 breaths per minute
Any noticeable increase in effort, even if rate is normal
👉 These changes often occur before obvious clinical signs and can be the earliest indicator of developing congestive heart failure
A Critical Clinical Point
Coughing does NOT equal heart failure
Coughing is one of the most commonly reported signs—but also one of the most non-specific.
Many dogs with DMVD also have concurrent respiratory conditions such as:
Tracheal collapse
Chronic bronchitis
Small airway disease
These are frequent causes of coughing, often more common than congestive heart failure in small-breed dogs.
At the same time, some dogs with true heart failure may have:
Minimal or no coughing
Increases in respiratory rate or effort
Why This Matters
Treating a cough as heart failure without confirmation can lead to inappropriate therapy
Missing early heart failure because coughing is absent can delay critical treatment
Monitoring RR/RE provides an early warning system at home
👉 Chest radiographs are required to confirm pulmonary edema, and echocardiography defines the underlying cardiac disease.
Advanced Treatment Options
Medical therapy remains the mainstay for most dogs, but advanced options are increasingly available for selected patients.
Transcatheter Edge-to-Edge Repair
A Minimally Invasive Option for Mitral Valve Disease
Transcatheter edge-to-edge repair (TEER) is an advanced, minimally invasive procedure designed to reduce mitral regurgitation in dogs with degenerative mitral valve disease. Rather than opening the chest, TEER is performed via a catheter-based approach on a beating heart, making it fundamentally different from open-heart surgery.
How the Procedure Works
The goal of TEER is to improve mitral valve closure by bringing the valve leaflets closer together.
A specialized device (e.g., V-Clamp) is delivered to the heart via a catheter
The device is positioned across the mitral valve under imaging guidance
The anterior and posterior leaflets are grasped and secured together
This creates a double-orifice valve, reducing backward blood flow
Result: Reduced mitral regurgitation and improved forward blood flow
Feasibility and Procedural Outcomes
Potter BM, Orton EC, Scansen BA, et al.
Clinical feasibility study of transcatheter edge-to-edge mitral valve repair in dogs with the canine V-Clamp device.
Frontiers in Veterinary Science. 2024
🔗 https://www.frontiersin.org/articles/10.3389/fvets.2024.1448828/full
“Procedural feasibility was 96%… Procedural safety was 96% based on survival to hospital discharge.”
Longer-Term Outcomes
Potter BM, Orton EC, Scansen BA, et al.
One-year echocardiographic follow-up and two-year survival in dogs undergoing mitral transcatheter edge-to-edge repair.
Journal of Veterinary Cardiology. 2025
🔗 https://www.sciencedirect.com/science/article/pii/S1760273425001328
“Mitral TEER resulted in sustained reductions in mitral regurgitation and left atrial size, with associated clinical improvement over time.”
These studies suggest that TEER is:
Technically feasible in appropriately selected dogs
Associated with high procedural success and survival to discharge
Capable of producing sustained improvements in mitral regurgitation and cardiac remodeling
At the same time:
Data are still emerging
Outcomes depend heavily on case selection and operator experience
TEER remains an advanced, referral-level intervention
TEER represents a promising, minimally invasive option for selected dogs with advanced mitral valve disease, with early data supporting both short-term safety and longer-term physiologic benefit.
Open-Heart Mitral Valve Repair
Open-heart mitral valve repair is currently the most definitive option for selected dogs with severe DMVD. It requires cardiopulmonary bypass and is available only at specialized centers. Candidate selection depends on size, stage, comorbidities, anatomy, cost, travel, and family goals.
Open-heart mitral valve repair is not widely available and is typically performed at specialized referral centers, including:
University of Florida Small Animal Hospital (USA)
Azabu University Veterinary Teaching Hospital (Japan)
JASMINE Veterinary Cardiovascular Medical Center (Japan)
École Nationale Vétérinaire d'Alfort (Maisons-Alfort, France)
Japan has been a global leader in veterinary mitral valve repair, with the largest number of cases and published outcomes.
Why See a Veterinary Cardiologist?
A heart murmur is just the starting point—it does not determine how serious the disease is or whether treatment is needed.
A veterinary cardiologist provides advanced diagnostics and precise staging, helping determine:
If heart disease is present
How advanced it is
When treatment should begin
How to Find One
Search for a board-certified cardiologist through the American College of Veterinary Internal Medicine (ACVIM):
👉 https://www.acvim.org/about-acvim/acvim-locator
You can also ask your primary veterinarian or contact a local specialty hospital.
A cardiologist helps move from uncertainty to a clear diagnosis, accurate staging, and a targeted plan.
Summary
Degenerative mitral valve disease is common, progressive, and often silent in its early stages. While a heart murmur may be the first clue, it is only the beginning—the most important step is determining where a dog is within the disease process.
Accurate diagnosis and staging allow for appropriate, evidence-based decision-making: monitoring early disease, initiating therapy at the critical Stage B2 window, and recognizing congestive heart failure based on objective findings rather than assumptions.
Clinical signs can be subtle and sometimes misleading. In particular, coughing alone does not diagnose heart failure, and over-reliance on this sign can lead to both over- and under-treatment. Instead, combining clinical assessment, echocardiography, thoracic radiographs, and home monitoring (such as sleeping respiratory rate) provides the most reliable approach to managing disease progression.
Advances in veterinary cardiology—from early medical intervention supported by the EPIC trial to emerging procedures such as TEER and open-heart mitral valve repair—continue to expand treatment options and improve outcomes.
With early detection, thoughtful monitoring, and stage-based care, many dogs with DMVD can maintain an excellent quality of life for years.
References
American College of Veterinary Internal Medicine Keene BW, Atkins CE, Bonagura JD, et al. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. Journal of Veterinary Internal Medicine. 2019;33(3):1127–1140. https://onlinelibrary.wiley.com/doi/full/10.1111/jvim.15488
Boswood A, Häggström J, Gordon SG, et al. Effect of Pimobendan in Dogs with Preclinical Myxomatous Mitral Valve Disease and Cardiomegaly (EPIC Study). Journal of Veterinary Internal Medicine. 2016;30(6):1765–1779. https://pubmed.ncbi.nlm.nih.gov/27678080/
Häggström J, Boswood A, O’Grady M, et al. Effect of pimobendan or benazepril hydrochloride on survival times in dogs with congestive heart failure caused by naturally occurring myxomatous mitral valve disease (QUEST Study). Journal of Veterinary Internal Medicine. 2008. https://pubmed.ncbi.nlm.nih.gov/19081392/
Borgarelli M, Buchanan JW. Historical review, epidemiology and natural history of degenerative mitral valve disease. Journal of Veterinary Cardiology. 2012. https://pubmed.ncbi.nlm.nih.gov/22386587/
Häggström J, Kvart C, Pedersen HD. Acquired valvular disease. In: Ettinger SJ, Feldman EC, eds. Textbook of Veterinary Internal Medicine.
Rishniw M, Erb HN. Evaluation of vertebral left atrial size (VLAS) as a method for assessing left atrial size in dogs. Journal of Veterinary Internal Medicine.
Buchanan JW, Bücheler J. Vertebral scale system to measure canine heart size in radiographs (VHS). Journal of the American Veterinary Medical Association. 1995.
Fox PR, Oyama MA, Reynolds CA, et al. Utility of NT-proBNP for identifying cardiac disease in dogs. Journal of Veterinary Internal Medicine. 2011.
Lalor SM, Gunn-Moore DA, Cash R, et al. Use of NT-proBNP in the assessment of cardiac disease. Journal of Small Animal Practice. 2012.
Potter BM, Orton EC, Scansen BA, et al. Clinical feasibility study of transcatheter edge-to-edge mitral valve repair in dogs with the canine V-Clamp device. Frontiers in Veterinary Science. 2024. https://www.frontiersin.org/articles/10.3389/fvets.2024.1448828/full
Potter BM, Orton EC, Scansen BA, et al. One-year echocardiographic follow-up and two-year survival in dogs undergoing mitral transcatheter edge-to-edge repair. Journal of Veterinary Cardiology. 2025. https://www.sciencedirect.com/science/article/pii/S1760273425001328
Uechi M, Mizukoshi T, Mizuno T. Mitral valve repair under cardiopulmonary bypass in dogs with degenerative mitral valve disease. Journal of Veterinary Cardiology.
Atkins C, Bonagura J, Ettinger S, et al. Guidelines for the diagnosis and treatment of canine chronic valvular heart disease. Journal of Veterinary Internal Medicine. 2009.
